Forearm fractures in children and adolescents are common injuries. Treatment of the radius and/or ulna (i.e. the 2 forearm bones) depends on the age of the patient, the location within these bones, and the amount of displacement. As a general rule, because younger patients have better remodeling potential of their fractures, less aggressive treatment strategies (i.e. casting with or without minimal manipulation) are necessary for uneventful healing. However, widely displaced fractures in the older adolescent may require maximum surgical intervention using plates and screws.
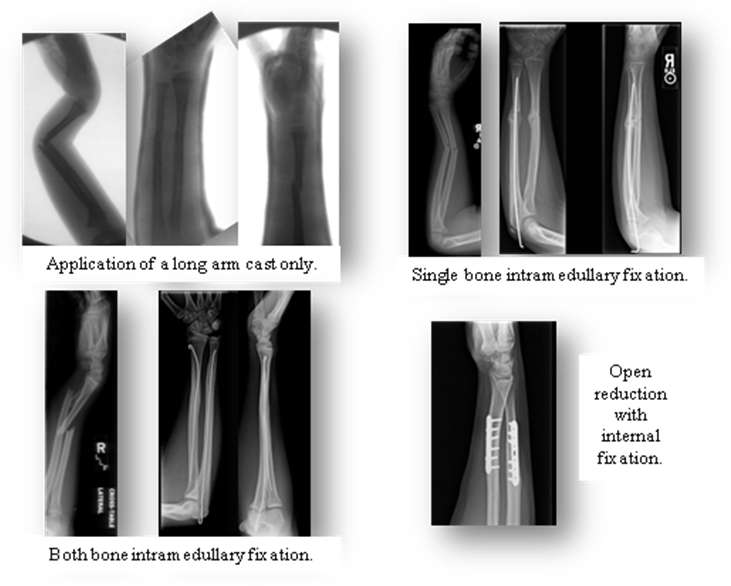
Frequently, general anesthesia is necessary to “set the bones” (i.e. reduce the fractures) and apply a well molded long arm cast to the patient’s forearm. Please note that safe induction of anesthesia requires an empty stomach. The initial cast often becomes loose as the swelling from the injury decreases, the muscles temporarily shrink due to disuse atrophy from immobilization, and the cast padding compresses over time. The deforming pull of the muscles in the forearm can lead to loss of initial alignment. Because we can predict which forearm fractures have a less favorable outcome with cast-only treatment, we sometimes recommend additional fixation. A minimally invasive technique using long, thin metal rods called “Intramedullary Fixation” is frequently used in the pediatric population. The decision to stabilize one or both bones, and whether to leave the rods exposed (with the intention of removing them in the office) or close the skin over the rods (with the likely need for surgical removal at a later time) are commonly made in the operating room.
The goal of surgical intervention of pediatric both bone forearm fractures is to restore function with most patients spending less than 6 weeks in a cast and returning to sports by 2-3 months.