
Bone Cyst of Foot Causing Pain
15 year old female presented for evaluation of activity related left heel pain of atraumatic origin for several weeks.

Radiographs revealed a large, well-circumscribed lucent lesion in the body of the Calcaneus.
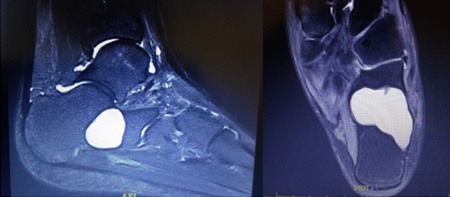
An MRI revealed a solitary cyst consistent with a Unicameral Bone Cyst (UBC). Given the size of the lesion and the thinning of the lateral Calcaneal cortex, pathologic fracture was a significant risk of observation.
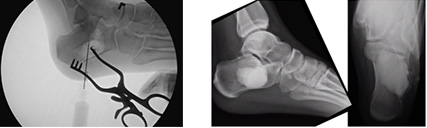
The patient went to the OR for a needle aspiration to confirm the diagnosis of UBC, followed by curettage and grafting with a synthetic bone graft substitute.

Three months later, the radiographs show partial resorption of the bone graft substitute, indicating bone ingrowth. The patient had returned to running sports without recurrence of pain.
Osteochondroma of Left Arm
12 year old male presented for evaluation of a slowly enlarging firm, but painless, mass on his left arm that was first noticed 3 years earlier. Clinical examination revealed no additional lesions on his body.

Radiographs of the left humerus revealed a large, pedunculated, solitary bony exostosis consistent with an osteochondroma. As this benign growth is anticipated to get bigger proportionate to the patient’s growth potential, surgical excision was offered.
Through a small incision, an osteotome was used to amputate the lesion at its base. Since its cartilaginous cap was removed intact, it would not grow back. The patient wore a sling for a week and returned to play after the skin incision healed.
Pathological Femur Fracture
10 year old male tripped and fell while visiting the Dominican Republic sustaining a right femur fracture. He was flown home and presented to the ER 5 days after the injury. The patient had no prior thigh/knee pain.

Radiographs revealed a displaced right distal femur femur fracture through a benign appearing bone lesion consistent with a Non-Ossifying Fibroma (NOF). NOFs are common in pediatric skeletons as they represent errors in formation of fibrous tissue, rather than bone, from the cartilaginous growth plates. Whereas most are small and asymptomatic and resolve spontaneously with growth, this one was large enough to compromise the integrity of the bone causing a fracture from a low energy mechanism.
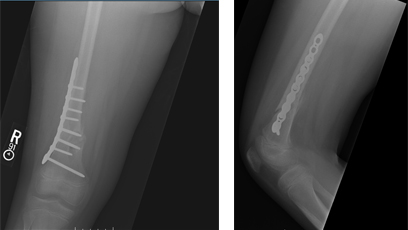
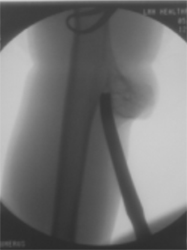
An open reduction and internal fixation was performed with a plate and screws. The NOF was curetted to stimulate healing and biopsy samples confirmed its benign nature.

Nine months later, once the fracture had completely remodeled and the NOF had significantly resorbed, the hardware was removed so as not to interfere with continued growth of the femur.
Ganglion Cyst of the Wrist
16 year old female with chronic complaints of left dorsal wrist pain and an area of swelling of atraumatic origin.
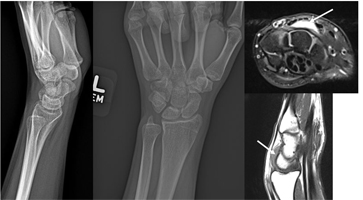
Radiographs of the left wrist were normal, but an MRI revealed a dorsal wrist ganglion cyst. As this was causing pain to the patient, she was offered an aspiration of the cyst in the office. Using a 30 gauge needle (the smallest needle we have), Lidocaine was used numb the skin overlying the cyst. Once numbed, a larger 18 gauge needle was used to aspirate the thick, clear gelatinous fluid that is characteristic of a ganglion cyst. Aspiration is associated with a significant risk of recurrence, but is an option for patients with symptomatic cysts whom are not ready for surgery. Unfortunately for this patient, the cyst, and pain, recurred. The patient underwent excision in the OR through an incision less than 1 inch in length and was immobilized in a wrist splint for 3 weeks. The cyst never came back and the patient’s pain resolved.
Toddler with Rheumatoid Arthritis of the Knee
3 year old male presents for evaluation a swollen knee. No injuries were reported and the patient has had no fevers. He is walking otherwise normally and has no significant pain.
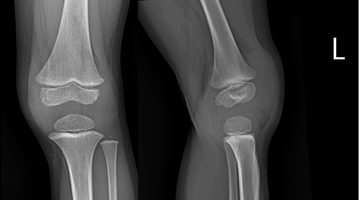
Radiographs revealed no acute osseous abnormalities, but significant soft tissue swelling corresponding to his clinical evaluation was appreciated. Blood work was performed and the patient was subsequently diagnosed with Juvenile Idiopathic Arthritis (JIA). Medical management under the direction of a Pediatric Rheumatologist ensued. However, a firm mass over the front of the left knee progressively enlarged over the next year.
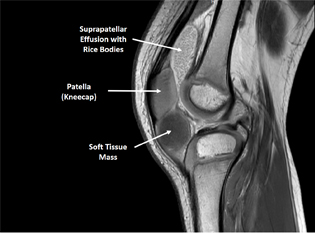
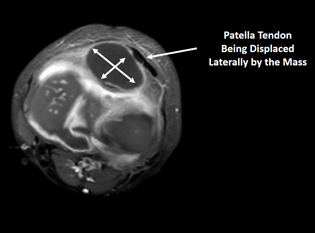
Due to his young age, an MRI under anesthesia was necessary to diagnose the mass. An excisional biopsy was performed and the mass was noted to be in the infra-patellar bursa (just outside the knee joint). The pathology came back as fibrinous material with hypertrophic synovium and chronic inflammation consistent with his diagnosis of JIA. The patient rapidly recovered from his procedure.
Bone Infection of a Child
4 year old female presented to the ER with a one week history of left “foot” pain and inability to ambulate associated with a fever. Over the past week, the patient was seen by her Pediatrician and at an Urgent Care, but was told to take Motrin for Transient Synovitis as she also had a cough. Upon examination, the patient refused to move her left ankle and there was generalized swelling to the lateral side. Initial radiographs of the foot and ankle were normal, but blood work confirmed elevation of her White Cell count and inflammatory markers. She was admitted for a STAT MRI of the Left tibia/fibula, but because of her young age, it would require anesthesia.
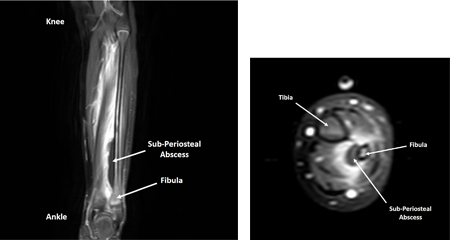
The MRI was reviewed in real time and confirmed the diagnosis of Distal Fibula Acute Hematogenous Osteomyelitis with a Sub-Periosteal Abscess. I informed the patient’s parents of the diagnosis and while still under anesthesia, the patient was brought to the OR for Irrigation and Debridement.

Through a small incision just above the growth plate, frank pus was encountered corresponding to the MRI findings. Samples were sent to the lab for Microbiologic analysis. The bone was decompressed with a curette (above image). Antibiotics were initiated and the patient was place in a boot to prevent an equinnus contracture of the ankle from developing. The patient responded appropriately. Her fever stopped and pain improved. The cultures grew Streptococcus Pyogenes (a bacteria commonly associated with Strep Throat) and she was discharged home on oral antibiotics.

The patient was walking less than 2 weeks after the procedure and was running by one month. She completed a 6 week course of antibiotics and follow up radiographs (see above) revealed a healthy growth plate.
Lyme Arthritis of the Knee Mimicking Septic Arthritis
7 year old female presented to the ER with a 2 day history of progressive, atraumatic swelling of the right knee. Low grade temperatures were present and the pain increased, limiting her ability to ambulate. Radiographs were normal, but blood work was mixed (normal White Cell count, but significantly elevated inflammatory markers). Because of the large joint effusion, the knee was aspirated (i.e. a sample of fluid was obtained after using Lidocaine with a tiny needle to anesthetize the skin). The synovial fluid was purulent in appearance and the resulting cell count had an extremely high White Cell proportion. Infection was the primary consideration and a STAT MRI was performed to rule out bone involvement. Although a Lyme titer was sent to the lab, this test does not generally result for 2-3 days.

As there was concern enough for possible Septic Arthritis (i.e. a spontaneous Bacterial infection that can rapidly destroy the articular cartilage of a joint), the patient was taken to the OR for an irrigation and debridement in the middle of the night. A quick procedure through a small incision on the outside of the knee allow copious irrigation with sterile saline and insertion of a drain to remove any additional fluid that may develop after. Antibiotics were initiated to cover typical organisms that cause Septic Arthritis in the pediatric population as well as for Lyme Arthritis. Two days after surgery, the patient was walking with minimal pain and remained afebrile. The drain was removed as no significant fluid re-accumulated. Nothing grew from the synovial fluid cultures and the Lyme titer finally returned with the diagnosis of Lyme disease. She was discharged home, feeling better, and continued her 28 day course of antibiotics for Lyme. Patient returned to gym/recess as the incision healed.
Foreign Body in the Foot
13 year old male was walking in socks when he stepped on a pencil and it impaled him in the bottom of the left foot.
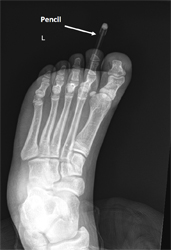
A radiograph of the foot demonstrates the pencil lodged deep in his foot. The pencil was removed by the ER physician, but the tip of the pencil was noted to be broken off. To evaluate for retained foreign body, a CT scan of the foot was performed.
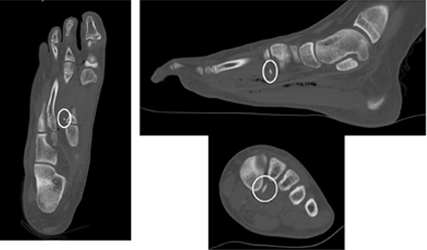
The CT confirmed retention of a radio-dense foreign body with dimensions consistent for the tip of a leaded pencil.
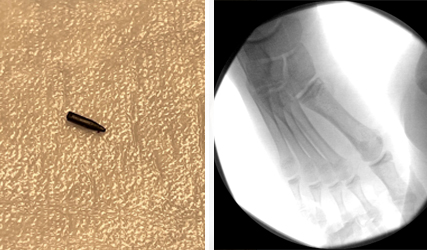
The patient was taken to the OR where a fluoroscopy machine was used to locate the foreign body. The pencil tip was removed in its entirety and confirmed fluoroscopically. The incision healed within 2 weeks and the patient returned to sports.
Osteochondroma of the Ankle
8 year old female noticed a firm mass on the anterolateral aspect of her right leg, just above the ankle. She was also beginning to complain of pain over it with running/jumping activities.

A radiograph of the right ankle revealed a large, sessile Osteochondroma of the anterolateral aspect of the distal Tibia with dystrophic changes to the adjacent Fibula.
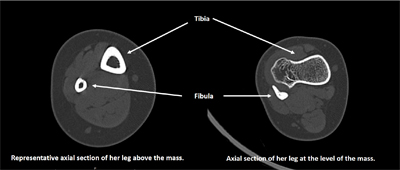
A CT Scan (see above) demonstrated the size of the Osteochondroma and how it was causing a mass effect on the adjacent Fibula.

Excision of the Osteochondroma was performed with the aid of intra-operative Flouroscopy (see above) to avoid iatrogenic injury to the distal Tibia growth plate. Drill holes traced out the anticipated resection area and the cuts were controlled with osteotomes. The patient was placed in a walking boot post-operatively and permitted to weight bear as tolerated.

The patient was back to gym and recess 1 month after surgery with no pain.