
“Functional” Scoliosis Resulting from a Limb Length Discrepancy
16½ year old female track athlete presented to her Pediatrician for evaluation of left sided low back pain. Radiographs were performed by her primary care physician and the radiology interpretation was that of an 18 degree apex left thoracolumbar Scoliosis. She was referred to Pediatric Orthopedics for further evaluation.
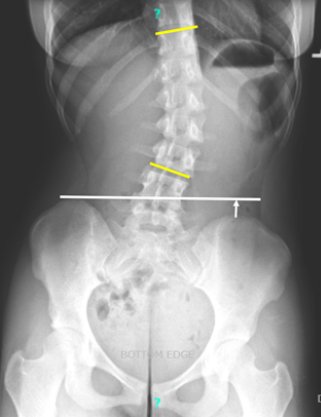
Upon independent review of her outside images, I noticed a significant limb length discrepancy as noted by depression of the left hemi-pelvis (white line/arrow above) in addition to the scoliotic curve (yellow lines). The left lower extremity was approximately 2/3 of an inch shorter.
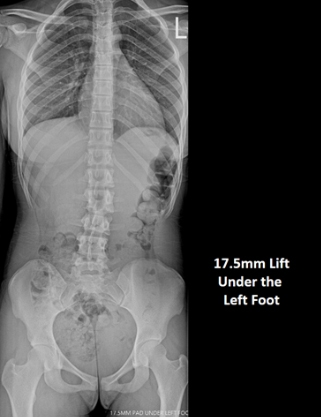
A new standing radiograph of the spine was performed with a 17.5mm lift placed under the (shorter) left foot. The effect of correcting for the limb length discrepancy can be seen above. As the patient is skeletally mature, a shoe lift to be worn inside her left sneaker was prescribed. Physical therapy was also recommended. Her low back pain improved, but the family was counseled that a permanent correction of her limb length inequality includes an acute shortening of the right femur or a small lengthening of the left femur.
Infantile Scoliosis Treated with Bracing
A 3 month old infant was brought in by his mother for evaluation of his spine. The patient was born premature at 34 weeks and was monitored in the NICU for weeks due to an intra-ventricular hemorrhage. Over the past month, mom had noted the patient had a preference to bend his trunk toward the right side. On exam, the patient had good tone in all extremities with no spasticity. While lying on his back, the patient assumed an apex left thoracolumbar position.

A supine radiograph confirmed a long thoracolumbar curve measuring 18 degrees.

At 6 months of age, the curve had progressed to 31 degrees. A custom Boston-style scoliosis brace was prescribed and the patient subsequently underwent an MRI, under sedation, of the brain and entire spine to rule out intra-spinal anomalies that can be associated with early onset scoliosis in curves over 20 degrees.
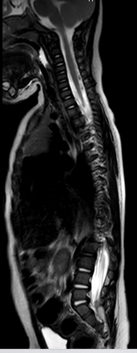
The MRIs revealed no intra-spinal anomalies and the brain component showed changes reflecting the perinatal stroke.

The radiograph above demonstrates the flexibility of his spine while wearing the brace. The patient began full time use of the scoliosis brace.
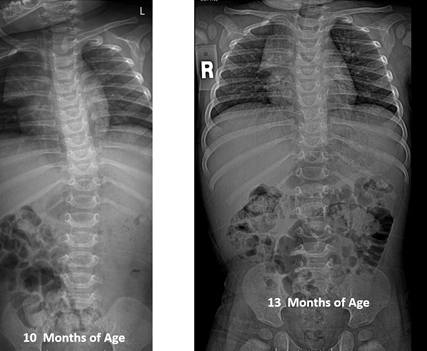
With continued full time use of the brace, the patient’s scoliosis resolved. Brace use was discontinued after 13 months of age and he was followed to ensure continued appropriate developmental gains.
Lumbar Spondylolysis in Adolescent Athlete
17 year old male presented for evaluation of new onset severe low back pain. No pains radiating down either leg. The pain began one week earlier after a competitive bowling tournament. No injury was reported.

On exam, the patient was tall (6’ 1”) and thin (160 lbs) and had markedly poor lumbar flexibility due to bilateral low back pain. The patient also had very tight Hamstrings. Radiographs (see above) were unremarkable, aside from mild asymmetry in the coronal plane. The patient was referred for an MRI to evaluate for a radio-occult Spondylolysis.
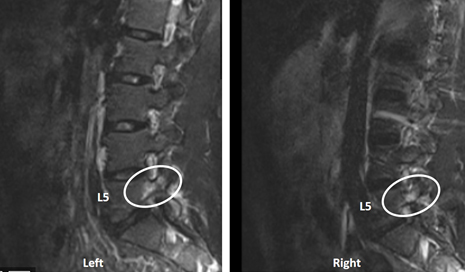
The MRI confirmed stress reactions in the bilateral L5 pars interarticularis/pedicles. Such pre-cursors to a stress fracture, known as Spondylolysis, are common in adolescents. Boys frequently have tight Hamstrings due to rapid growth in the pubertal years, and a lack of emphasis on stretching. The tight Hamstrings limit pelvic motion with activities, putting more stress on the L5-S1 junction. Spondylolysis is also common in adolescent girls, but their cause is more frequently associated with repeated lumbar hyperextension activities (ex. Tumbling in cheer or gymnastics).
This patient rested from sports/activities, wore a soft lumbar corset that limited lumbar extension during the daytime, took Ibuprofen as needed for pain, and began a physical therapy and home exercise program consisting of core strengthening and regular Hamstring stretches. The patient’s pain resolved quickly and improved lumbar range of motion followed. He returned to competitive bowling 8 weeks after his evaluation.