
Developmental Dysplasia of the Hip in a Newborn
A newborn girl was noted to have bilateral hip instability following a C-Section for Breech presentation. Examination revealed an Ortolani positive right hip and a Barlow positive left hip.
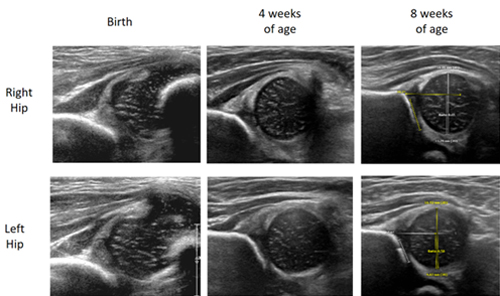
The initial ultrasound of the hips revealed the right side was worse than the left, but both were abnormally developed. The patient was placed in a Pavlick Harness prior to discharge home from the hospital with instructions for full time use. A follow up ultrasound at 4 weeks revealed improvement in the right side and near normal left side. By 8 weeks of treatment, both hips had normalized and the patient weaned use of the harness to 12hrs/night for 2 weeks and then discontinued its use.
Slipped Capital Femoral Epiphysis (SCFE) – Hip Problem Masquerading as Chronic Knee Pain
A 10 year old female presented for evaluation of chronic right knee pain. Approximately one year earlier, the patient was treated with antibiotics following a tick bite. At around the same time, the patient’s onset of right knee pain was attributed to Lyme’s disease. She remained active in sports including martial arts and soccer, but the pain persisted. Evaluation of the right knee was unremarkable, but the patient had limited range of motion of the right hip.
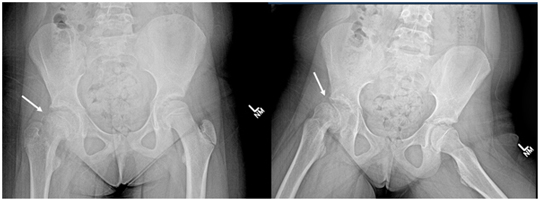
Radiographs of the pelvis revealed a moderately severe, but stable, Slipped Capital Femoral Epiphysis (SFCE). SCFE occurs when the proximal femoral growth plate fails, causing a deformity of the hip and can manifest as hip, thigh, or knee pain and altered gait.
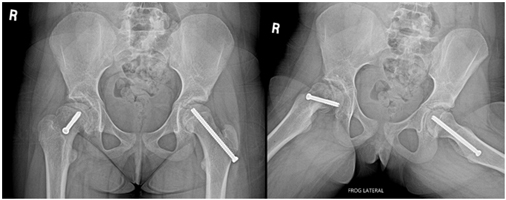
In Situ fixation of the right hip stabilizes the slipping growth plate. Due to her young age, she was at significant risk of this happening on the left side, and prophylactic screw fixation was performed at the same time. The patient’s “right knee pain” resolved immediately following the surgery. Post-operatively, the patient was allowed to walk on the left side, but toe touch weight bearing was encouraged on the right side for the first 4 weeks. The patient returned to sports at 2 months.
Knee Pain/Clicking from a Symptomatic Discoid Lateral Meniscus
8 year old male presented for evaluation of atraumatic right knee clicking and popping associated with pain. Examination revealed the pathology to be coming from the lateral compartment.
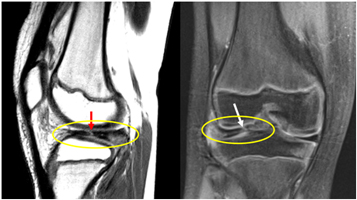
Xrays were unremarkable, but a follow up MRI revealed a complete Discoid Lateral Meniscus (Yellow ovals) with a tear (Red and White arrows). A Discoid Meniscus is a congenital abnormality in the knee that a patient is born with. They generally present with symptoms of pain or instability as the patient grows. Due to the patient’s mechanical symptoms, arthroscopic surgery was offered.
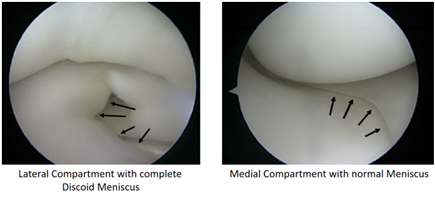
A diagnostic arthroscopy was performed, confirming the Discoid Lateral Meniscus (note the normal appearing Medial Meniscus).
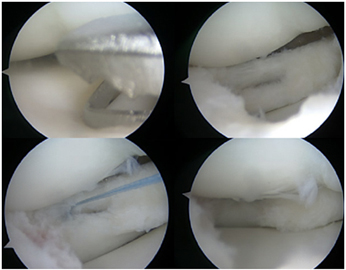
A “Saucerization” was performed. Using a meniscal biter and shaver, the redundant portion of the central Discoid Lateral Meniscus was removed (i.e. partial meniscectomy), exposing a horizontal tear in the posterior horn that was repaired with an all-inside suture device. Post-operatively, the patient was ambulating with a brace by the first week and began physical therapy. By 4 weeks, the patient was cleared to resume gym/sports/recess.
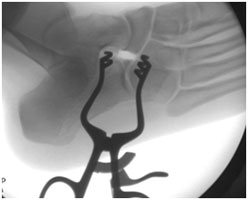
Baby Born with an Extra Thumb
Infant presented with an isolated congenital deformity of the right hand. A duplication of the thumb is seen clinically and radiographically.
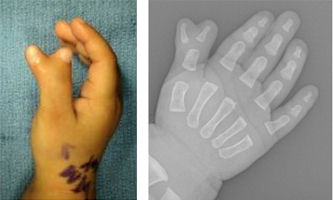
Excisional reconstruction was offered at 1 year of age.
Intra-op fluoroscopic image confirms the appropriate level of resection of the extra thumb.

Function was preserved at follow-up.
Baby Born with an Extra Toe
Infant was born with an extra toe on the left foot. Polydactyly of the foot is associated with shoe wear issues as the child ages and excisional reconstruction was offered at 1 year of age.

Extra Bone in the Foot Causing Pain
11 year old male presents as a second opinion for chronic right foot arch pain. Treatments by a Podiatrist including orthotics were unsuccessful at alleviating his pain with activities of daily living.

Examination revealed the patient had bilateral flexible flatfeet, but with pain to palpation over the right Navicular prominence that was replicated with active resisted Posterior Tibialis Tendon function. Radiographs revealed an Accessory Navicular. Resection of the extra bone was offered to alleviate his pain.

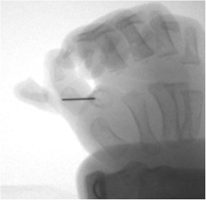
The Posterior Tibialis Tendon was split, exposing the Navicular prominence. An intra-operative Flouroscopic image with a needle confirmed the location of the pseudarthrosis (i.e. false joint) and the Accessory Navicular was completely removed. Post-operatively, the patient was progressed to weight bearing as tolerated in a walking boot, underwent early physical therapy, and had pain resolution by 6 weeks.
Congenital Dislocation of the Knee
Newborn infant was born with a hyperextension deformity of the left knee.

The left knee could not be flexed and initial radiographs revealed a dislocation of the knee joint. An ultrasound of the hips revealed normal development.
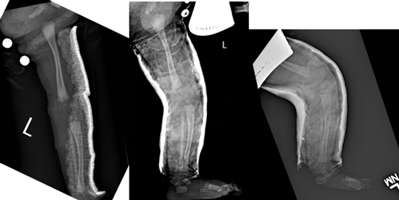
Initially, a long leg plaster splint was applied (above left) to limit hyperextension. Then, serial casting (above middle and right) was performed to gradually stretch the contracted quadriceps mechanism. After 4 weeks, the patient was placed in a Pavlick Harness to maintain the reduced position of the flexed knee for an additional 4 weeks.
Polysyndactyly of the Foot Causing Toe Deformity with Growth
8 year old male presented for progressive deformity of the right 4th toe. Another orthopedist recommended orthotic use when he was younger for a congenital abnormality of his right foot. However, as he grew, the 4th toe progressively assumed a more and more flexed position, akin to a hammer toe).

An extra toe (polydactyly) had partially developed between the native 4th and 5th toes, which were also webbed (syndactyly). The larger 4th toe was tethered to the smaller 5th toe and growth had forced the 4th toe into a flexed posture. The deformity was predicted to get worse with growth and excisional reconstruction of the Polysyndactyly was recommended.
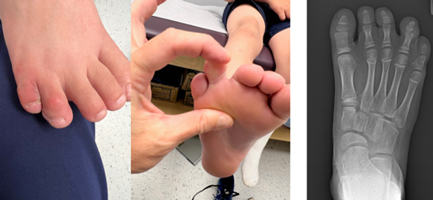
The “6th toe” between the 4th and 5th toes was removed and skin flaps separated the 4th and 5th toes to allow independent growth. Clinical pictures and a radiograph is shown above at 2 months post-operatively.
Curly Toe Causing Progressive Deformity and Pain
6 year old male with pain and deformity of the left 4th toe. Since birth, the patient’s left 4th toe was bent under the 3rd toe, causing pain with shoe wear. Radiographs revealed normal osseous structures.

The patient underwent a left 4th toe flexor tenotomy (i.e. release of the tight tendon) and a “Z”-plasty to lengthen the chronically contracted plantar skin.

The patient wore a boot for the first two weeks after the procedure to protect the incisions and returned to gym by 3 weeks with improved clinical alignment of the 4th toe (see above photos).
Tarsal Coalition Causing Chronic Foot/Ankle Pain
15 year old female twisted her ankle and continued to have foot/ankle pain despite rest, boot immobilization, physical therapy, and nonsteroidal anti-inflammatories.

Radiographs reveal a Calcaneo-Navicular Tarsal Coalition (congenital abnormal connection between two bones in the foot) that restricted normal subtalar range of motion.
The family elected for surgical resection of the coalition. Post-operatively, the patient was weight bearing in a boot and resumed physical therapy. The patient was pain free by 2 months after surgery and was cleared to resume all activities.
Congenital Pseudarthrosis of the Distal Fibula Causing Chronic Ankle Pain with Sports
13 year old male with chronic, atraumatic lateral ankle pain with running sports. After being seen by a General Adult Orthopedist, he was referred to an Orthopedic Oncologist for a biopsy of “irregular bone” causing pain. Results of the biopsy were normal, but the patient continued to have pain and dysfunction with activities. Parents sought a third opinion. This time with a Pediatric Orthopedic Surgeon.

Xrays and CT revealed a fracture non-union with atrophic features and post-surgical changes from the prior biopsy.

Open reduction and internal fixation was supplemented with Iliac Crest (pelvis) bone graft to aid in his fracture healing.

The patient was ambulating, pain-free, in a boot by 1 month post-op and was cleared to return to sports by 2 ½ months post-op. The patient was subsequently diagnosed with a rare condition called Congenital Pseudarthrosis of the Fibula, explaining his unusual fracture and bone quality.
Bilateral Clubfeet Discovered on Pre-Natal Ultrasound
The parents just had a routine pre-natal ultrasound and were surprised by the results. Their second child will have bilateral clubfeet. Without an appointment, they came to office for a consultation. I reviewed the standard of care for Idiopathic Clubfeet; the Ponsetti Method. Reassured that their baby will have a proper start at life, I next saw them back after he was born.

Over the course of several weeks, Mom and Dad brought him in to the office for weekly casting to progressively stretch both feet. This culminated in a minimally invasive procedure in the OR to lengthenboth Achilles.

After the final cast was removed, bracing was necessary to prevent recurrence until, and even after, he started to walk (on time).

Routine follow up visits ensured he continued to growth and develop normally.

He is doing great and loves to play baseball!
“We can never begin to thank you for all you have done for him. Looking back at those baby pictures is crazy. You made this journey easy for scared stressed parents from the moment I met you walking into the office pregnant with no appointment. You overheard me talking to the front desk and you pulled me into an office and explained the process. Thank you again.” – Patient’s Mother
***Clinical pictures and quote are included with the permission of the family.
Crooked Finger after an Injury One Month Earlier
12 year old male, right hand dominant, “jammed” his rightlittle finger playing basketball and presented 2 ½ weeks later to a Hand Surgeon with a “crooked finger”, but resolved pain. The Hand Surgeon recommended seeing a Pediatric Orthopedic Surgeon.
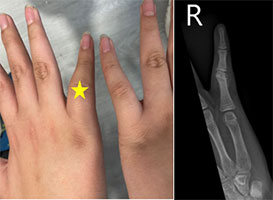
The patient had an abduction deformity of the right little finger and radiographs revealed a mal-uniting proximal phalanx neck fracture.

Pre-Op planning is critical as the finger is small and correction is critical.

Through an incision just over half an inch, the osteotomy is accomplished, and correction is maintained with 2 pins that will be removed in the office after being in a cast for 4 weeks.
Lower Extremity Limb Length Inequality
11 ½ year old male presented for evaluation of “uneven hips”.
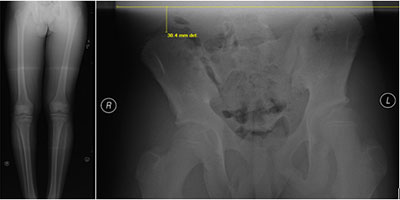
Standing radiographs revealed the left lower extremity was approximately 3cm longer than the right lower extremity. An assessment of the patient’s potential growth remaining indicated that slowing the growth on the long (Left) side could allow the short (Right) side to “catch up”.
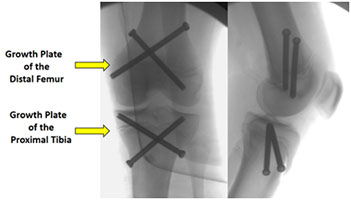
A minimally invasive procedure called Epiphysiodesis introduced 4 screws, each through an incision approximately 1 cm in length, crossing the growth plates around the left knee to halt future growth. The patient returned to sports and activities within 1 month and was followed until skeletal maturity.
Bowlegged Knees
12 year old male presented for evaluation of “Bowleggedness”.

A standing joint survey radiograph of the bilateral lower extremities revealed bilateral proximal tibialvarus deformities. Persistent bowleggedness into adulthood is associated with premature knee osteoarthritis. Since the patient was still growing, they were offered “Guided Growth”.

In Guided Growth, small plates/screws are inserted over the growth plate to slow growth on one side, thereby allowing the opposite side to catch up. After several months of growth, the radiographs reveal normalization of the lower extremity mechanical axes. If the patient is still growing, the plates need to be remove to prevent over-correction into “Knock-Knees”.
Toddler with a “Bent” Thumb
2 year was noted by the mom to be unable to extend her right thumb for “some” time. Clinical evaluation revealed the inability to extend the interphalangeal joint of the right thumb, but the left thumb had normal range of motion.

Radiographs revealed normal development of the bones with sign of injury. Note that the thumb is flexed in the radiograph. The patient was diagnosed with a Congenital Trigger Thumb. Pediatric patients can develop triggering of fingers for reasons that are different than in adults, and are treated primarily surgically.
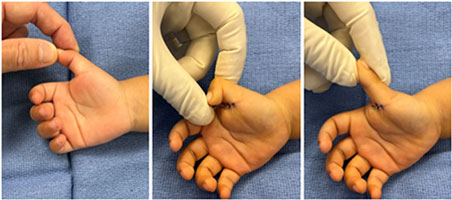
The clinical pictures show the extent of thumb extension pre-op. Through an incision less than 1cm in length and taking less than 10 minutes, full range of motion has been restored. Three absorbable sutures are placed and a soft bandage is kept in place for 1 week. The child can use the hand immediately post-operatively for play.
Birth Trauma Cases
The process of delivering a newborn can be traumatic for the mother and/or the baby. The goal is to expeditiously deliver the infant so as to avoid neurologic events associated with prolonged deliveries.
Clavicle fractures frequently occur during a vaginal birth because the infant’s shoulder can get stuck on the mother’s pelvic bone. By fracturing, the clavicle briefly shortens thereby allowing the baby to pass through the birth canal quicker. Also by fracturing, it poses less risk of stretch to the Brachial Plexus (the complex network of nerves that exit the neck and heads down the arm.

Fortunately, Clavicle fractures in newborn heal and reliably remodel rapidly (above left image reveals a displaced mid-shaft left clavicle fracture on the day of birth and the above right image reveals copious callus formation by 2 weeks of age).
The second most common birth trauma fracture is of the Humerus (i.e. the arm bone). Gentle traction on the baby’s upper extremity is sometimes necessary to assist extraction, but can result in a fracture.
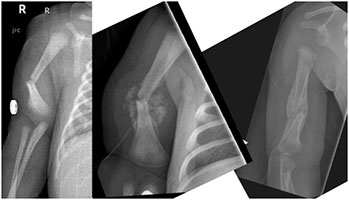
By simply using a Bobby pin to hold the wrist portion of a long sleeve shirt to the opposite shoulder as an “Infant Sling”, the arm is immobilized for no more than two weeks (central xray with copious fracture healing). By 2 months (right xray), the deformity has remodeled normally.

A device used to treat infants with hip dysplasia (i.e. Pavlick Harness) immobilizes the leg and after only 3 weeks (right xray), there is abundant healing of the fracture.

By 2 months of age, extensive remodeling is already noted.

By 2 years of age, there is no evidence of the birth fracture and the standing xray reveals symmetry of the mechanical axis and limb length of the lower extremities.