
Rotational and angular deformities of the lower extremities are common concerns of parents that result in the Pediatrician’s referral to a Pediatric Orthopedic Surgeon.The rotational and angular alignment of a child’s lower extremity changes significantly with growth. Intra-uterine molding of the developing child influences the position of the hips, legs, and feet.
Intoeing (aka Pidgeon Toe) is often first noticed by parents when a baby begins walking, and walking “well” is present in 90% of children by the age of 15 months. When mild, intoeing may cause parental concern simply by the appearance, but in the extreme, it may cause functional impairment such as excessive tripping and falling. Fortunately, it rarely causes pain and the vast majority of intoeing represents the spectrum of normal variability with anticipated spontaneous resolution. Children at various ages may display intoeing for different reasons. There are 3 reasons a child walks with the toes pointed toward the midline.
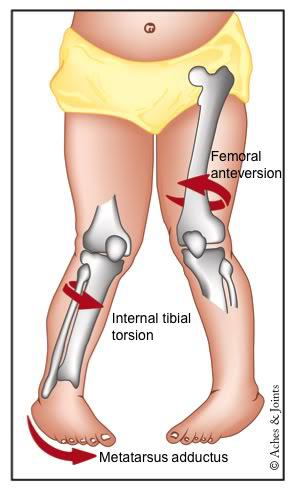
- “Twisted Thigh Bone” known as Femoral Anteversion represents excessive internal rotation of the femur at the level of the hip. This is a frequent cause of intoeing in the 4-7 year range and is more common in girls. Most children outgrow this by the time they reach 10 years of age and there are no braces that can effectively accelerate spontaneous improvement. Rarely, surgical “De-rotation” is performed in the older child with persistent impairment.
- “Twisted Shin Bone” known as Internal Tibial Torsion represents excessive internal rotation of the tibia. This is common in the newborn and is attributable to the necessary “packaging” of the legs in the uterus. It usually resolves spontaneously by the age of 3, and like femoral anteversion, no braces effectively expedite this process. Internal Tibial Torsion frequently makes a child’s leg look more bowlegged than it really is.
- “Curved Foot” known as Metatarsus Adductus represents a “bean”-shaped foot that is present at birth and due to pressure on the foot when developing in the mother’s uterus. Mild forms may improve spontaneously or with simple stretching, however some require casting or bracing to more effectively stretch the foot. Surgery is sometimes required in the older child.